
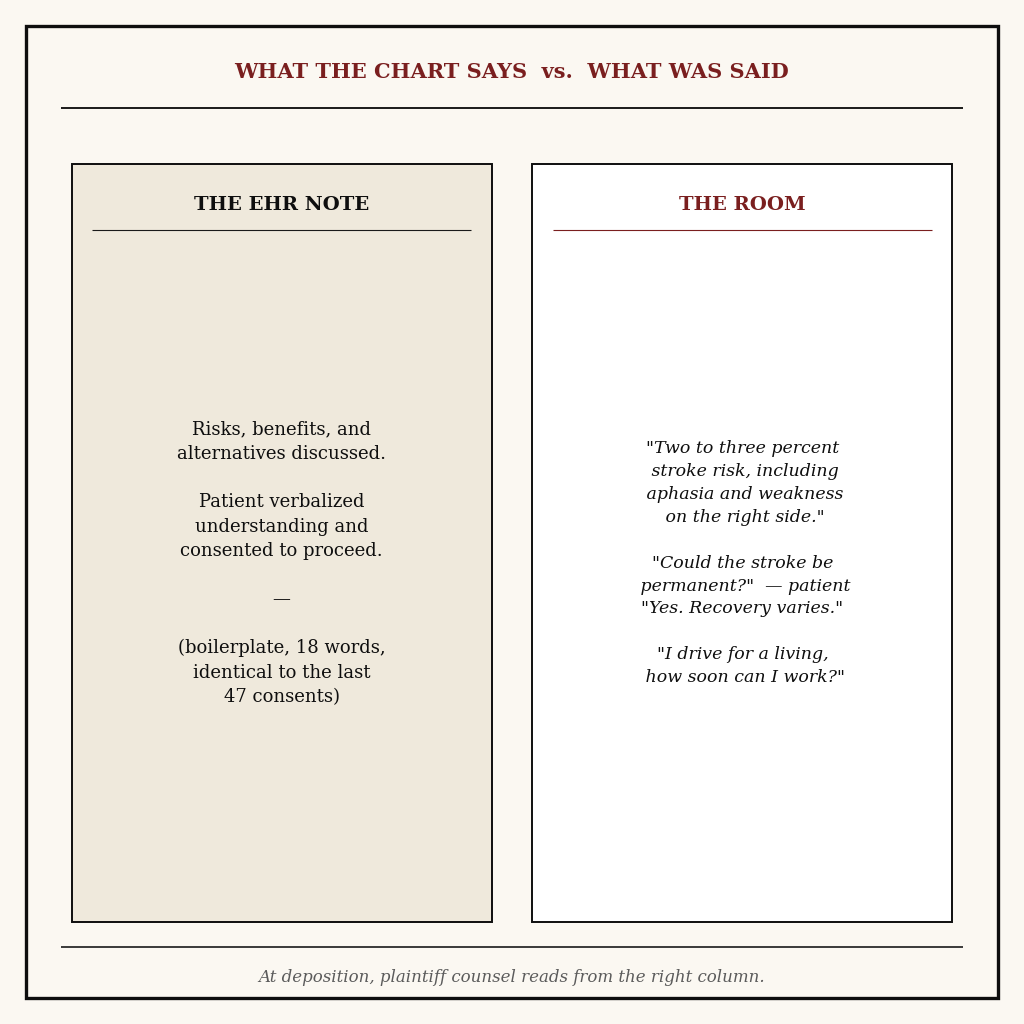
The boilerplate sentence is the most expensive line in surgical documentation. It satisfies the consent form. It checks the EHR field. And in a deposition room eighteen months later, it sits on the page next to the plaintiff's testimony like an apology written before the harm. Every plaintiff malpractice attorney in the country knows the sentence by heart. So does every defense attorney, which is why the defense attorney's first question to the surgeon, in preparation, is some version of "what else did you actually say?"
That question is the entire problem. The surgeon said a great deal — fifteen to thirty minutes of specific, careful, patient-tailored disclosure — and none of it lives anywhere except in the surgeon's memory. Memory deteriorates. The chart does not.
The Preop Conversation Has No Stenographer
Surgical informed consent is a fifteen to thirty minute discussion that has to satisfy three audiences at once. The patient, who must actually understand what is going to happen. The signed consent form, which is precise about the procedure name and vague about everything else. And a future jury, who will weigh whether disclosure met the reasonable patient standard in the jurisdiction.
The verbal exchange is where consent actually happens. The patient asks about returning to a job that requires lifting, about driving in two weeks, about the dominant hand, about what happens if the lump turns out to be malignant. The surgeon names specific complications — stroke for carotid endarterectomy, anastomotic leak for colectomy, ureter injury for hysterectomy — and quotes incidence numbers in plain language. None of that lands in the chart.
When a complication occurs and the case turns on what was disclosed, the plaintiff argues that the specific risk that materialized was never named. The defense brings the surgeon's memory, the pre-printed form, and the boilerplate sentence. Against a patient who plausibly testifies that no one mentioned that risk, that stack rarely wins.
What the Reasonable Patient Standard Actually Requires
Most U.S. jurisdictions have moved from the older "reasonable physician" standard to a reasonable patient standard for informed consent. The question at trial is not what most surgeons would have disclosed; it is whether a reasonable patient in this patient's position would have wanted to know the specific risk that materialized — and whether that disclosure actually happened in language the patient could understand.
That standard asks a question the boilerplate sentence cannot answer. "Risks, benefits, and alternatives discussed" does not name the risk. It does not establish that the disclosure was in plain language. It does not show that the patient's specific questions — the lifting job, the dominant hand, the recovery timeline — were answered. The defense theory has to be reconstructed from the surgeon's memory of a single conversation among hundreds.
Why Current Solutions Fail
Pre-printed consent forms list common risks, but the patient signs without reading and the surgeon initials without modifying. Voice memos on a personal phone are a HIPAA problem and never get transcribed. Hospital scribes are not in the preop area for outpatient cases and most ambulatory surgery. The EHR consent template that says "I discussed risks A, B, C and the patient verbalized understanding" is hard-coded and never reflects what was actually said.
Even surgeons who free-text more detail do it from memory, hours later, between cases. The note describes a generic discussion, not the specific one with this patient about the patient's specific job and specific questions. At deposition, generic is what loses.
Risk-management teams know this. Defense attorneys know this. The reason nothing changes is that every alternative previously proposed — bring a scribe into preop, install a recorder, write a longer note — fails either the cost test, the workflow test, or the HIPAA test. The result is an industry-wide acceptance that the most legally vulnerable conversation in surgery is also the most poorly documented.
What Actually Works
The legally protective record is the one that captures specific language. Not "discussed stroke risk" but "explained two to three percent stroke risk including aphasia and right-sided weakness, patient asked whether the stroke could be permanent, I answered yes and that recovery varies."
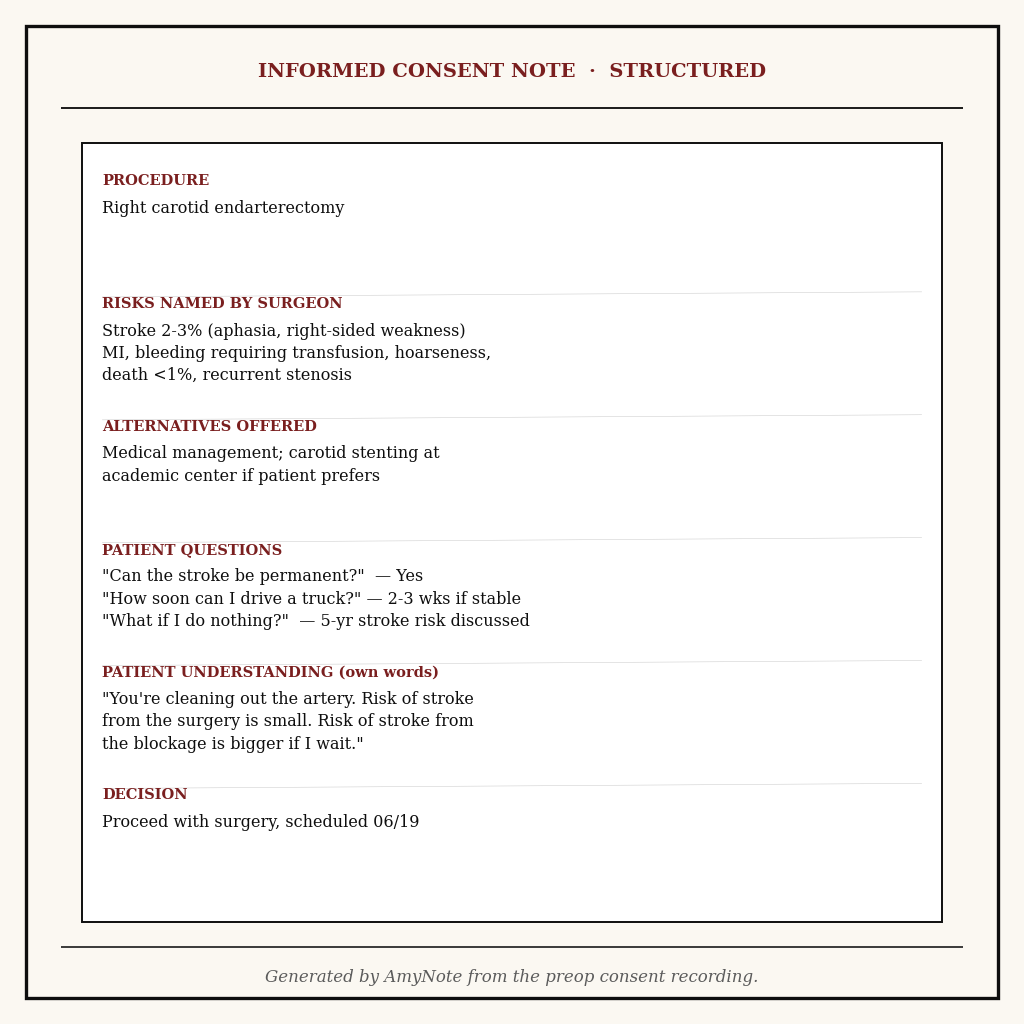
AmyNote records the preop consent discussion on the surgeon's iPhone or laptop, transcribes the audio with OpenAI's Speech API running through the surgeon's own account, and uses Anthropic's Claude Opus to produce a structured Informed Consent Note: the specific risks the surgeon named, the verbatim incidence numbers stated, the alternatives offered, every question the patient asked and the answer given, the patient's stated understanding in their own words, and the final decision. Names and medical record numbers can be redacted before any file leaves the device.
Both OpenAI and Anthropic contractually guarantee zero training on user data. Audio is encrypted in transit; processing copies may be retained to deliver and recover requested features. Transcripts stored locally on device with encrypted transport. The audio file itself can be retained for the local statute of limitations window if risk management asks for it, or destroyed immediately after the note is signed.
At deposition the surgeon does not have to remember. The note quotes what was actually said, in the patient's words and the surgeon's words. The jury reads a contemporaneous record of a careful, specific conversation. The plaintiff theory that the risk was never disclosed has to clear a much higher bar.
What the Structured Consent Note Captures
The post-encounter summary that lands on the surgeon's screen mirrors the structure a malpractice defense attorney would build from scratch if given the transcript:
- Procedure named and indication. What is being done and why, in plain language, in the order the surgeon explained it.
- Specific risks disclosed with incidence. Each named complication and the percentage or descriptor the surgeon used — "two to three percent," "rare but serious," "less than one in a thousand" — preserved verbatim.
- Alternatives offered. Watchful waiting, medical management, less invasive procedures, declining surgery entirely — including the ones the patient rejected and why.
- Patient questions and surgeon answers. The specific concerns this patient raised — return to work, driving, the dominant hand, anesthesia history — and what was said in response.
- Stated understanding. The patient's own words confirming they understood, captured rather than paraphrased.
- Decision and timing. Whether the patient consented immediately, asked for time to think, or wanted to speak with family first.
HIPAA, BAA, and the Compliance Conversation
The reason cloud transcription tools have struggled to enter the preop workflow is that hospital compliance teams will not approve audio of a HIPAA conversation sitting on a third-party server with a generic terms of service. AmyNote's posture answers that question directly: audio is encrypted in transit; processing copies may be retained to deliver and recover requested features on provider servers, and transcripts live on the surgeon's own device with encrypted transport. Both OpenAI and Anthropic operate under Business Associate Agreement frameworks and contractually guarantee zero training on customer data.
For the risk-management review, that means the chain of custody for the audio file is short and auditable. The audio exists only on the device that recorded it. The transcript is generated and stored on the same device. If the case is closed and the statute of limitations runs out, the file is deleted by the same hand that created it.
Getting Started
For a surgical practice the workflow is unchanged. The surgeon starts AmyNote at the beginning of the consent discussion, obtains the patient's verbal acknowledgement that the conversation is being recorded, lets it run, and stops at the end. The structured note is ready by the time the surgeon walks back to the workstation. The surgeon reviews, edits anything the transcription missed, and signs into the chart alongside the standard consent form.
The protective value is in the specificity. Try AmyNote on the next ten consents and put those notes next to the standard template. The difference is what risk managers and defense attorneys have been asking surgeons to produce for years — and the boilerplate sentence, kept in the chart alongside the new record, finally has the context it always needed.
Originally published as an X Article.


